Trigeminal Neuralgia
Information for those affected
Trigeminal Neuralgia
Information for those affected
1. Definition
Trigeminal neuralgia is a facial pain syndrome strictly confined to the areas supplied by the branches of the trigeminal nerve. It is caused by damage to the nerve in this region, almost always triggered by external stimuli. The condition is characterized by extremely severe, sudden attacks of pain that recur in bursts, separated by intervals of complete pain relief. As the disease progresses, the intervals between attacks become shorter.
2. Symptoms
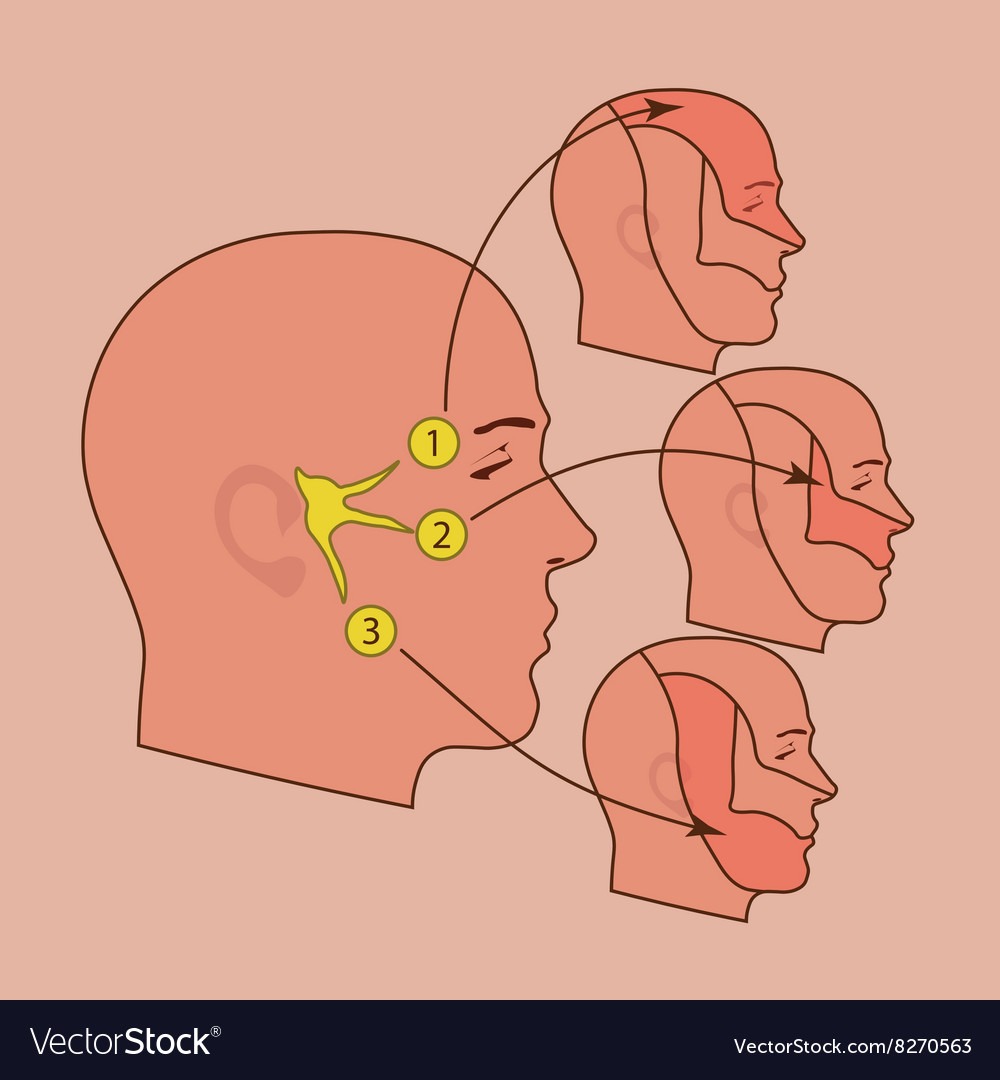
The affected structure is the fifth cranial nerve, the trigeminal nerve, which consists of three branches. Most commonly, the second or third branch is involved — the upper jaw, lower jaw, and mouth.
Key characteristics:
- Pain occurs lightning-fast, is extremely intense, and lasts from seconds to a few minutes.
- It is triggered by external factors such as cold air, eating, chewing, tooth brushing, or washing the face with cold water. These external triggers are called triggering.
- Reflexively, the facial muscles often contract due to the pain; therefore, the condition is also known as tic douloureux.
- Usually, only one side of the face is affected.
-
Common Misdiagnosis
Because the pain radiates into the upper and lower jaw, trigeminal neuralgia is often mistaken for a dental problem. This unfortunately leads to situations where patients have multiple teeth removed before finally seeing a neurologist.
Conversely, trigeminal neuropathy can occur after tooth extraction — but the pain pattern is fundamentally different: neuropathy causes constant pain without lightning-like attacks.
-
Symptomatic Forms
Tumors or vascular processes in the posterior cranial fossa, herpes zoster, and skull base fractures can cause pain similar to trigeminal neuralgia.
Multiple sclerosis can also lead to demyelination of the nerve or brainstem, resulting in trigeminal neuralgia — often even on both sides.
In all these cases, lesional procedures are the treatment of choice.
-
Atypical Forms
Typical trigeminal neuralgia must not be confused with trigeminal neuropathy. Neuropathy causes constant pain that usually cannot be triggered externally.
It may arise from nerve injury (e.g., trauma, root canal treatment) or neuroma formation after dental or jaw procedures.
Important: Neuropathy must not be treated with lesional procedures. Neurostimulation is one possible treatment option.
3. Cause
The exact cause of trigeminal neuralgia is not fully understood. A commonly discussed mechanism is compression of the nerve at the brainstem by a crossing blood vessel. The pulsations of this vessel may lead to local demyelination, causing short circuits within the nerve. These aberrant impulses are perceived as pain.
4. Therapy
There are numerous therapeutic options for trigeminal neuralgia — reflected in more than 3,000 publications since 1966.
The optimal therapy depends on many subjective and objective factors and must be discussed thoroughly with the treating physician. A second opinion is often advisable.
Treatment Methods
-
Medications
- The most effective drug is carbamazepine (Tegretol, Neurotop).
Dosage must be increased slowly due to side effects. Once an effective dose is reached, it should be maintained long-term.
- If carbamazepine is ineffective or poorly tolerated, diphenylhydantoin may be tried.
- Alternatives: valproate, clonazepam.
- Conventional painkillers (NSAIDs, opioids) are generally ineffective.
-
Infiltration
Local anesthetic injections into peripheral nerve branches may provide temporary relief but are not suitable as long-term therapy.
-
Percutaneous Thermocoagulation
One of the most frequently performed and best-studied procedures.
Principle: pain-conducting C-fibers are less myelinated and therefore more heat-sensitive.
Procedure:
- Performed under short anesthesia.
- A special probe is guided to the Gasserian ganglion under X‑ray control.
- Position is confirmed with electrical stimulation while the patient is awake.
- The ganglion is heated to 70°C for ~90 seconds, selectively destroying pain fibers.
Hospital stay: ~2 days.
-
Balloon Compression
Similar goal as thermocoagulation but uses a small balloon inflated within the ganglion to destroy pain fibers.
Less selective; used in centers without thermocoagulation capability.
-
Glycerol Injection
Instead of heat, glycerol is injected into the ganglion to denature nerve tissue.
-
Microvascular Decompression (MVD)
Microvascular Decompression (MVD)
Considered the first-choice surgical treatment, especially when the first branch or all three branches are affected.
Principle:
- The nerve is compressed by a crossing vessel.
- During surgery, the posterior fossa is opened, the trigeminal nerve is exposed, and the vessel is gently moved away.
- A small Teflon pad or muscle piece is placed between nerve and vessel.
Advantages:
- The only method that preserves the nerve and can cure the disease.
Disadvantages:
- Requires craniotomy and longer hospital stay.
- Recommended mainly for patients under 70 years.
-
Radiosurgery (Gamma Knife, LINAC)
A non-invasive lesional procedure using focused radiation.
Pain relief occurs only after several months.
Long-term results are still limited.
5. Diagnostic Findings
Diagnosis is usually based on the characteristic symptoms.
MRI is routinely performed to exclude other causes such as tumors or vascular malformations.
6. Frequency
- Typically occurs after age 45.
- Affects about 40 per 100,000 people.
- Female-to-male ratio: 3:2.
7. Further Information
If you have questions or are affected yourself, the site offers personal consultation.
Contact: info@trigeminusneuralgie.at